What Outcomes Can Patients at Foundation Psychology Expect?
When engaging a service to help with your wellbeing, it’s crucial to have a clear understanding of the potential outcomes. That’s why here at Foundation Psychology we’ve conducted research on our patient’s journey throughout therapy. We sought to answer the simple question:
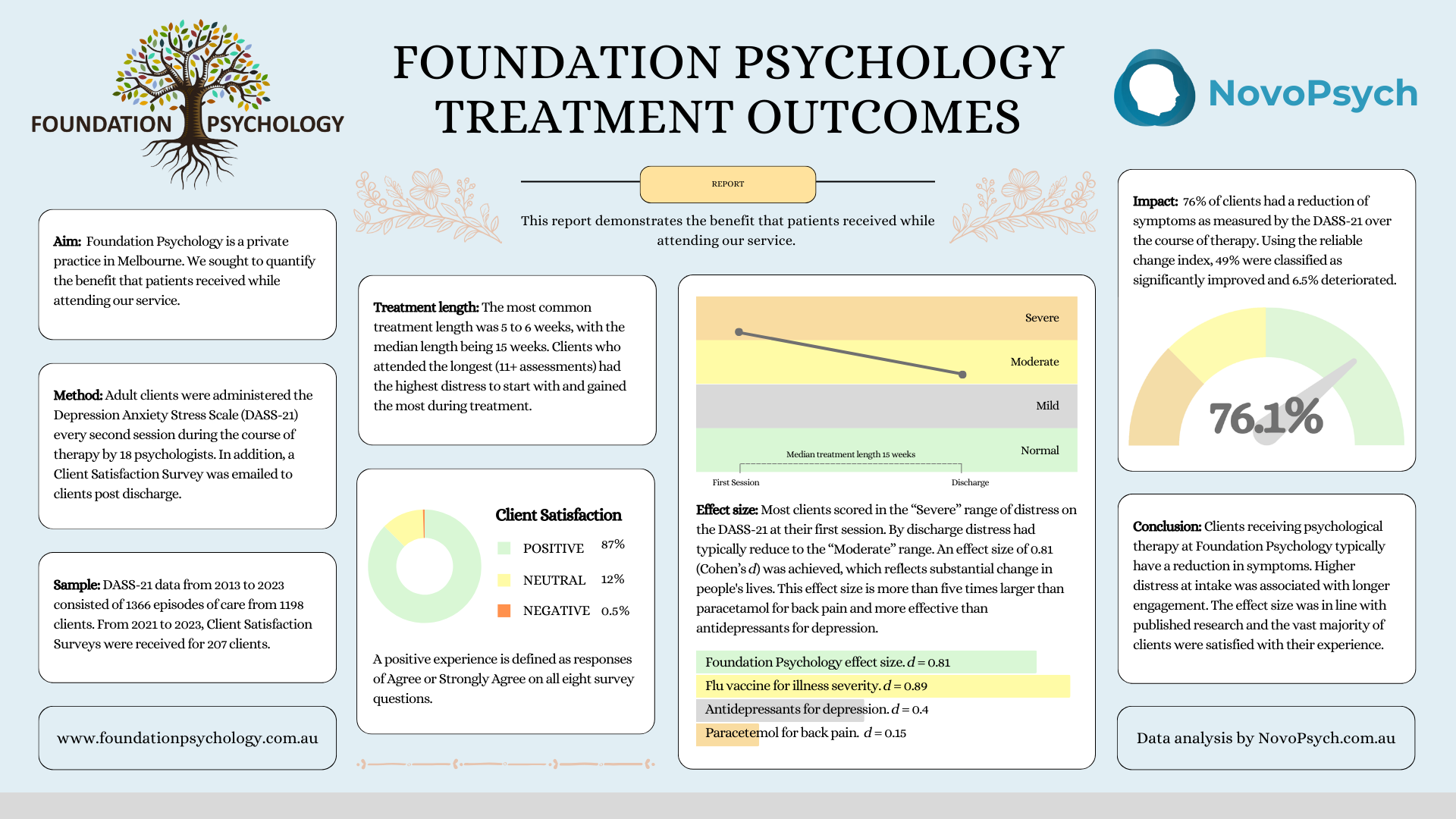
What proportion of clients experience improved well-being during the course of therapy?
Our psychologists are trained to help with many issues, such as improving self-understanding, coping strategies, enhancing relationships and treating mental disorders such as anxiety and depression. While there is no easy way to measure everything that our psychologists can help with, there are two broad ideas that we systematically measure to quantify the success of a patient’s journey during therapy.

1. Psychological Distress is a term used to describe a range of emotional and mental difficulties individuals may experience. It encompasses feelings of sadness, anxiety, stress, and depression, and can manifest in both mental and physical symptoms. Psychological distress is not a clinical diagnosis in itself but is often a sign or symptom of many mental health conditions. By measuring psychological distress with a questionnaire called the DASS-21 at the start, middle and end of therapy, we can quantify the level of change in distress over time.

2. Client Satisfaction is arguably the most important construct to measure, as it encompasses the patient’s sense of their overall experience at Foundation Psychology. The Client Satisfaction Survey is provided to patients at the end of therapy, and gives us a sense of how the patient felt about the quality of care, the therapeutic relationship, service delivery and quality of life improvements.
Results


When considering the question of “how much” benefit therapy produced, it can be helpful to contextualise the results in comparison to other well established treatments. To do this, we computed the standardised effect size (Cohen’s d), which represents the standard deviation between DASS-21 scores at the start and end of treatment. An effect size of 0.81 is five times more effective than paracetamol for back pain and more than three times the effect on happiness when doubling of someone’s income!


Treatment Length
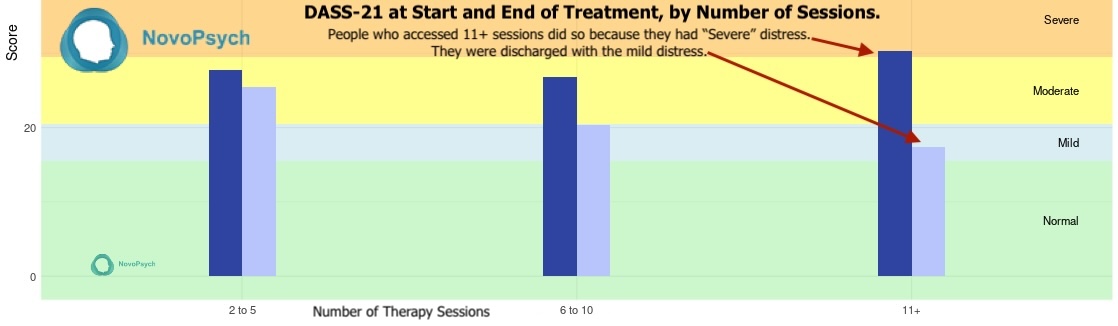
The most common treatment length was 5 to 6 weeks, with the median length being 15 weeks. Clients who attended the longest (11+ sessions) had the highest distress to start with and gained the most during treatment. This indicates that longer engagement in therapy produces better results.
Conclusion
The majority of clients receiving psychological therapy at Foundation Psychology had a reduction in symptoms. This is great news, and indicates we’re providing high quality care.
While everyone’s therapeutic journey is individual and we are certainly not professing to be able to fully capture our patient’s complex lives with these numbers, it provides us with an evidence-based set of expectations about Foundation Psychology.
The results of our study are comparable to other published research about the benefit of psychological services. For example, Study 4 of the comprehensive Better Access Evaluation found that between 44-55% experienced significant improvements in well-being, and Study 2 found a little over half of people accessing care experienced reduction in symptoms. Using a similar metric as this evaluation called the “reliable change index”, 49% of clients had “clinically significant” improvement in the Foundation Psychology sample.
Part of our commitment to patient care is engaging in continual professional development. Therefore, we will benchmark ourselves against these results annually and tweak our service to enhance care even further.
For more details read below
Method and Sample
Foundation Psychology uses NovoPsych, an outcome monitoring platform to collect and analyse this data. Adult clients were administered the Depression Anxiety Stress Scale (DASS-21) every second session during the course of therapy by 18 psychologists between 2013 and 2023. An episode of care was included if there were two or more DASS results within a six month period and the first score was above 15. This cut-off point for the first score meant that only clients who were classified as “mild” distress or higher in the first assessment were included. The rationale for this was that if someone scored below this level then the DASS-21 was not likely to be an appropriate measure for the client’s presenting issue. As in, it wasn’t capturing and measuring their specific problem. Over this period, DASS-21 data from 1,366 episodes of care from 1,198 clients was included.
A Client Satisfaction Survey was emailed to clients post discharged from 2021 to 2023. During this period 207 responses were collected. The response rate was less than 20%.
Limitations
Like all research, this study had a number of limitations. Firstly, our sample was restricted to adult clients, so we don’t have good visibility on the outcomes for children and their families attending our service. Measuring outcomes among young people has methodological complexities which were outside the scope of this research.
In addition, this research did not include a comparison group such as a wait-list control, so the proportion of change in DASS-21 scores caused by therapy itself cannot be quantified. Mean reversion and extra-therapeutic factors such as life circumstances may have had an influence over levels of distress.
A further limitation was our data collection method. While it was the practice’s policy to collect DASS-21 data every second session, this meant that the full change in symptoms would not have been captured if an assessment was not administered in the first and final session. In addition, some psychologists were not collecting outcomes with the routine and rigour specified in our method. These limitations in our dataset likely underestimated the real level of therapeutic change achieved. In future iterations of our outcome analysis we hope to address this methodological shortcoming.